Acid Reflux Teeth Damage: The GERD-Dental Connection

Most people who have acid reflux or GERD think of it as a stomach or throat problem. The connection to dental health is less obvious but just as real: stomach acid that reaches the mouth, even briefly, is far more concentrated than the acid in food or drink, and repeated exposure silently erodes the enamel on the back surfaces of the teeth in a pattern that is distinctive, progressive, and irreversible once significant structure is lost. Understanding acid reflux teeth damage and its dental implications is important for anyone managing GERD, because protecting the teeth requires a different set of habits than treating the reflux itself.
At Willow Family Dentistry in Wylie, TX, Dr. Esther B. Jeong identifies GERD-related erosion patterns at routine exams and works with patients to protect what enamel remains while they manage their condition with their physician.
How Does Acid Reflux Damage the Teeth?
Acid reflux damages teeth when stomach acid, with a pH of approximately 2, reaches the mouth and dissolves enamel on contact. The damage is intrinsic, meaning it comes from inside the body, making it more concentrated and harder to buffer than dietary acid erosion.
Acid reflux damages teeth through the same mechanism as dietary acid erosion, but with a critical difference: stomach acid has a pH of approximately 2, far more acidic than coffee, soda, or citrus fruit. When stomach acid reaches the oral cavity through reflux or vomiting, it lowers the mouth's pH well below the critical threshold of 5.5 at which enamel begins to dissolve. Repeated exposure means the enamel is being challenged by an extremely potent acid, often without the patient realizing it is happening.
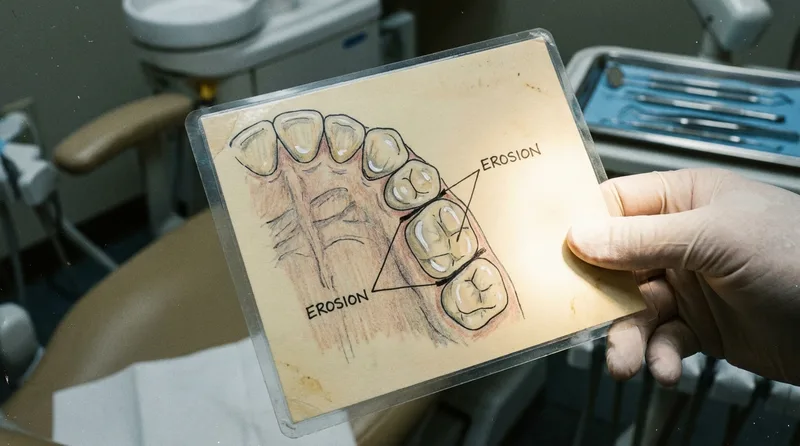
GERD-related erosion affects teeth in a characteristic pattern that dentists are trained to recognize. The upper back teeth, particularly the palatal surfaces, the surfaces facing the roof of the mouth, tend to show the most damage because acid pools in the back of the throat and flows across those surfaces when a person is lying down. The front teeth may show a glassy, translucent appearance along the edges as enamel thins, and the back chewing surfaces can develop a cupped or dished appearance as the softer dentin beneath the enamel is gradually exposed.
According to research published in peer-reviewed dental literature, patients with GERD have a significantly higher prevalence of dental erosion compared to controls, with some studies finding erosion rates 3 to 5 times higher in reflux patients than in controls, according to that body of evidence. The condition is often silent from the patient's perspective until significant damage has accumulated.
Why Is Nighttime Reflux Especially Damaging to Teeth?
Nighttime reflux is especially damaging because saliva flow drops dramatically during sleep, removing the mouth's primary acid buffer. Acid that reaches the teeth at night stays in contact far longer, and lying flat increases both frequency and duration of reflux episodes.
Nighttime reflux is especially damaging to teeth because saliva flow drops dramatically during sleep, eliminating the mouth's primary defense against acid. During the day, saliva continuously neutralizes acid, washes it away, and provides minerals that help remineralize early-softened enamel. At night, this protection is largely absent, meaning acid that reaches the teeth during sleep stays in contact with enamel far longer before being cleared.
According to WebMD, lying flat removes the gravitational advantage that keeps stomach contents below the esophageal junction during the day, making nighttime reflux episodes both more common and more prolonged than daytime ones. For the teeth, this means more acid exposure per episode and longer contact time with enamel that has no saliva defense available to minimize the damage.
Patients with GERD who sleep flat are at higher risk than those who elevate the head of their bed. Even a modest elevation of six to eight inches reduces the frequency and severity of nocturnal acid exposure. This is worth raising with a physician when discussing GERD management, both for esophageal health and for the teeth.

What Does GERD-Related Tooth Erosion Look Like?
GERD erosion follows a pattern that dentists recognize: glassy palatal surfaces on upper back teeth, translucent front tooth edges, and cupped or dished molar cusps. This pattern reflects where reflux acid pools when a person lies down, and it differs clearly from dietary erosion patterns.
GERD-related tooth erosion has a distinctive pattern that differs from erosion caused by dietary acid alone. Dietary erosion tends to affect the front surfaces and biting edges of the teeth. GERD erosion primarily affects the palatal surfaces of the upper teeth, the chewing surfaces of the back teeth, and occasionally the lingual surfaces of the lower front teeth. This pattern reflects where refluxed acid contacts the teeth when a person is lying down.
Early signs visible to a dentist include a smooth, glassy appearance on the palatal surfaces of the upper incisors and premolars, slight transparency at the incisal edges, and subtle cupping or dishing on the cusps of the back teeth. As erosion progresses, teeth may appear shorter, more yellow as the enamel thins and the yellower dentin shows through, and increasingly sensitive to temperature and sweet stimuli.
In significant cases, existing fillings may appear to rise above the surrounding tooth surface as the enamel around them erodes away, since composite and amalgam do not dissolve in acid the way enamel does. This is a telling clinical sign. Our guide on enamel erosion causes and prevention covers how this pattern of damage compares to other types of erosion and what the restoration options are once significant loss has occurred.
How Can You Protect Your Teeth if You Have GERD?
Protecting teeth from acid reflux damage requires managing the reflux itself, modifying a few specific habits around acid exposure, and using fluoride to strengthen enamel between episodes. Together these substantially reduce the rate of erosion even in patients with active GERD.
Protecting teeth from acid reflux teeth damage requires a combination of managing the reflux itself, modifying a few specific habits around acid exposure, and using fluoride to strengthen enamel between exposures. None of these steps eliminates risk entirely in someone with active GERD, but together they substantially reduce the rate of erosion and can preserve enamel for many years that might otherwise be lost.
The most important protective habits include:
- Do not brush immediately after a reflux episode. Acid softens enamel temporarily, and brushing within 30 to 60 minutes of acid exposure abrades softened enamel. Rinse with water or a dilute baking-soda solution first to neutralize the acid, then wait before brushing.
- Rinse with water or a fluoride mouthwash regularly, especially in the morning after a night of potential reflux, to clear residual acid and support remineralization.
- Elevate the head of your bed to reduce nocturnal reflux episodes, which are the most damaging to the teeth due to low saliva flow during sleep.
- Use a prescription-strength fluoride toothpaste if your dentist recommends one based on the degree of erosion present. Standard over-the-counter fluoride provides some protection, but higher concentrations offer more remineralizing benefit for patients at elevated risk.
- Stay well hydrated to support saliva production, which is the mouth's primary buffering mechanism against acid throughout the day.
- Work with your physician to manage the GERD effectively. Dental protection against acid reflux teeth damage is adjunctive; the most important intervention is reducing the frequency and severity of acid exposure at its source.
Our article on sudden tooth cold sensitivity covers how enamel loss from any source, including GERD, progresses to the point of sensitivity and what can be done at each stage.

Should You Tell Your Dentist About GERD?
Yes. Sharing your GERD diagnosis with your dentist allows them to watch for early erosion patterns, recommend appropriate fluoride, and track changes over time. Many patients omit GERD from dental history forms because they do not connect reflux to oral health.
Yes. Sharing your GERD diagnosis and current management with your dentist allows them to watch for early erosion patterns at checkups, recommend appropriate fluoride treatments, and flag any changes in the erosion picture between visits. Many patients do not think of GERD as a dental health issue and omit it from medical history forms, which means the dentist is working without important context when interpreting what they see in the mouth.
According to Healthline, GERD affects an estimated 20% of the US population, making it one of the most common chronic conditions a dental office encounters in adult patients. Awareness of the dental implications of GERD is important both for the patient and for the dental team.
If you have GERD and have not had a dental checkup recently, an exam is a good opportunity to assess the current state of your enamel and discuss protective strategies. If erosion is already present, early intervention with remineralizing agents and fluoride is far simpler than the restorative work needed once significant enamel loss has occurred. Our article on gum recession touches on a related crossover condition, since acid-related gum tissue changes can accompany enamel erosion in some GERD patients.
Can Tooth Erosion From GERD Be Reversed?
Tooth erosion from GERD cannot be fully reversed once significant enamel has been lost, since enamel does not regenerate. Very early surface mineral loss can be partially reversed with fluoride and remineralizing treatments, but visible structural damage requires restorative dentistry.
Tooth erosion from GERD cannot be fully reversed once significant enamel structure has been lost. Enamel does not grow back. However, very early erosion, at the stage of surface softening and mineral loss before visible structural change, can be partially reversed through remineralization with fluoride and calcium phosphate treatments. This is why catching and managing erosion early makes such a significant difference to the long-term outcome.
When erosion has progressed to the point of visible structural loss, the options shift to protective and restorative dentistry. Dental bonding can cover and protect affected surfaces. Veneers or crowns may be appropriate for more significantly eroded teeth. Our article on teeth grinding and jaw damage is relevant here too, since bruxism and GERD often coexist and the combination produces enamel loss at a significantly faster rate than either condition alone.
Willow Family Dentistry helps patients at every stage of this process, from early monitoring and prescription fluoride for active GERD with minimal erosion, to discussing restorative options for patients whose enamel has already been significantly affected. The goal is always to preserve as much natural tooth structure as possible for as long as possible.
Managing GERD and concerned about your teeth?
Book an evaluation at Willow Family Dentistry in Wylie, TX. Dr. Jeong will assess your enamel for erosion patterns, discuss protective strategies, and work alongside your physician's GERD management.
Explore preventive dentistryFurther Reading
GERD-related dental erosion connects to a broader set of conditions affecting enamel and oral health. The articles below go deeper on related topics.
- Toothache at Night: Why It Gets Worse and What to Do
- Dry Mouth at Night: Causes, Risks, and Solutions
- Mouth Breathing and Teeth Damage: Causes and Solutions
Results may vary. Please consult with Dr. Jeong for personalized treatment recommendations.
Dr. Esther B. Jeong, DDS
DDS · Willow Family Dentistry
Wylie family dentist with 15+ years of experience providing gentle, judgment-free dental care.
Frequently Asked Questions
Was this article helpful?
You may also like



Have a dental question?
Schedule a consultation and get personalized answers from Dr. Jeong.
Call us
(972) 881-0715
Hours
Mon – Thu: 9am – 5pm
Fri: By Appointment
Location
1125 W FM 544, Wylie
Emergency? Same-day appointments available.